Search the Community
Showing results for 'alcohol'.
Found 17,501 results
-
Another Christian here. I don't think God minds if people turn to medical help in dealing with alcohol or drug addictions...or cigarette addictions. My thought is, why should food be treated any differently? If there is medical treatment available, and it leads to better health for you, I do not see a conflict in your faith. I see it as very different than plastic surgery for purely vain purposes. I am not a very good scripture-quoting person, but have strong faith. I hope perhaps some of this makes sense.
-
How miserable to not lose any weight in a year. I really feel for you. Yes I would go to a therapist and find out how to stop the emotional/addictive eating. You can do it! I have given up alcohol, drugs and cigarettes in my lifetime. I go to a 12 step group and it really helps me. Did you get any nutritional classes before you were banded? We got quite a few hours of instruction and it really helped me to understand why my body needs healthy food. Good luck!
-


Not Telling People....
O.T.R. sleever replied to JPSnAZ's topic in POST-Operation Weight Loss Surgery Q&A
Umm, sure it is. We have already proven to ourselves (and everybody else) that we dont have what it takes to stick to the diet & exercise thing on our own. Many of us have tried every other gimmick under the sun to lose weight, and failed. We are food addicts (most of us anyhow). If there were a surgery that could cure alcohol, drug, gambling, or porn addictions would there be any objections to using those surgeries? I think not. We have a weakness when it comes to food. Therefore we NEED help. We need this to be as "easy" as it can be. And let me tell you, after over 6 months with my sleeve, when your stomachs capacity is 6-8oz total, it's pretty damn easy to not eat a 16oz steak, or a whole pizza, or 4 slices of cheesecake. When someone makes the remark "that's the easy way" I have to agree. Last I checked we are always searching out easier ways of doing almost everything. Cars are so much easier than bicycles The Internet is easier than encyclopedias Tractors are easier than a horse & plow Debit cards are easier than writing checks or carrying cash Pre prepared foods are easier than scratch cooking Since when is making something easier a bad thing? -
Hi everyone--so far I am staying on track, now that I am finally back to exercising. The cough will not go away, I sure do wish it would, I am very ready to breath normally again!!! Yesterday, we went out and cut 3 trees for the Christmas party at DH's work. We walked out in the hills for miles it seemed!!! But it was great fun, the weather was cool and clear, and we saw HUGE jackrabbits, and several deer, and a coyote. We found the trees we wanted, and then the work began!!! DH was insistant I would learn how to chop these trees!!! Let me add, the area we went to get the trees is on BLM (Bureau of Land Management) and it was tagged. You could only cut tagged trees, because they were being thinned, and culled for burn protection. So if people didn't cut them for Christmas, they were going to be removed, and debranched in January/February. They remove all branches under 8" and leave the trunks in piles, for people to gather as fire wood. The branches are mulched back into the ground. So anyway we cut 3 trees, and it was WORK!!!! Then we had to carry them back to the truck. We had a wonderful time!! I had been worried about DH, we had been at odds, and I was worried he was dealing with some depression, but he was his old self yesterday---what a relief!!! We were gone all day, it literally took hours to get the trees carried back. We had stopped and got Subway (I know.....) to take out with us, and we had several jugs of water. He has a winter emergency kit in the truck, with canned goods, candles etc. I know I got my exercise in yesterday!! Today I will use my energy trying to remove the sap from my hands!!! Not really, but I bathed them in alcohol yesterday getting it off. Today he and the guys will get them in stands, and the party staff will take over. At first I was kinda irritated that he had to be the one to go out and get them. Seems like he always gets the extra things to do....but afterwards, I am VERY glad he did---it was a great day!!! Today I have been to Curves, and am heading out to buy 3 things...and then I am done. Well I have baking and junk to do, but that is it---Bring it on Christmas, I am ready!!! Hope everyone has a great day!!!! And if you stop in Heather (K@t) !!!!HAPPY BIRTHDAY!!!!! Hope your day is special! Kat
-
Anyone lose friends after Lap Band?
MichelleBee replied to angelic3432's topic in POST-Operation Weight Loss Surgery Q&A
I chose to sever ties with my best friend of 7 years. She is diabetic, will not take care of herself, and can't stop eating or drinking alcohol, I had tried to help her on numerous occasions, I told her please don't end up like an ex of mine that almost died from diabetes because he would not take care of himself, I also asked her to please stop drinking, for her own health, and I told her that she was seriously hurting herself. At the end of our relationship, she was the biggest I had ever seen her, seriously, she was bigger then me. After my lap band, our relationship changed a lot, It seemed like her whole LIFE was centered around getting food, eating food, or securing food for later. I couldn't eat much of anything after my surgery, and at restaurants when I would go to eat with her, she would try to make me eat. She was trying to sabotage me, and I actually let her one time. I was so angry that I let her make me feel that bad, that I ended our friendship. If she wants to be fat and unhappy, let her be, sometimes you cannot help people help themselves. -
Why no alcohol?
-
Call your surgeon's office and ask why you can't have caffeinated coffee or tea. My only restriction was no soda and it was advised to avoid alcohol. Welcome!
-
I've read many threads about caffine not being allowed, but my nutritionist says coffee and tea are fine. At first, I guess you want to use your limited stoma space for the most nutritious foods, since liquids wash things through. Also, I've read about alcohol affecting banders faster and I wonder if this is true for caffine. I don't drink much soda at all, so giving it up isnt an issue for me. I have also read about people drinking "flat" soda OK.
-

Telling people, Judgements, and Accountability with the Band
we3601 replied to tarajim's topic in POST-Operation Weight Loss Surgery Q&A
Well, you can definitely add me to the None of Your Business Camp. Besides the medical staff, the only person that knows is my husband. I've read the other posts where people tried to keep it semi-secret and you have only confirmed my fears. Someone always "swears" someone else to secrecy and then it's common knowledge. I struggled with the decision as far as telling my two sons (18 & 23) but decided it might be information they may tell their girlfriends, friends by "accident," and then I'm in the same situation where people that I don't want knowing my business end up knowing. Unfortunately, WLS is judged by society and not in a positive light. I, myself, feel that I have taken a very, very extreme measure in the fight of obesity. I can't help but sometimes wish I had the "power" to lose weight with proper diet and exercise and not with the aid of a tool. I am an alcoholic in recovery and have been sober almost 2 years so this may just be part of my problem, too. Admitting my food addiction may be even harder than admitting my addiction to alcohol. I am new to this lapband process so perhaps in time, I will be able to share this news in the future. But for now -- mums the word. I also don't know how successful I am going to be so telling others about this extreme measure and then failing would be devastating. PS: I do sometimes remind my husband that he is the ONLY person who knows and that if it ever gets out, I'll know where to go "Soprano Style." -
You can have lots of things. It just depends on how you want to spend your calories. But as an occasional treat, I'm sure these are not the worst choice out there. But beware, Atkins products use a lot of sugar alcohols and a lot of people get dumping with them.
-
I hear you! I am 4 weeks post op now and I have 2 mantras: "I'M NEVER GOING BACK!" and "IT's JUST NOT WORTH IT!" (when tempted to taste or take a bit of something not allowed.) This is way too much work, money, and risk to throw it away. Use this pre-op time to really clean up your eating. After surgery, you want every bite to be as nutritionally dense as possible, and as healthy as possible. The "New you" deserves nothing less. Get rid of the artificial sweeteners, colors and flavorings. Get rid of the soda and caffeine. (Caffeine may come back later, but you may find you feel better and more stable without it and really not want it anymore. I LOVED coffee, but can't even stomach the thought of it now!) Absolutely get rid of the sugar! ALL sugar! Get rid of processed food. Cook it yourself. Get rid of simple carbs/starches. Minimize wheat or get rid of it altogether. Learn to enjoy other whole grains like quinoa, brown rice, millet, teff, amaranth. Learn to enjoy veggies - LOTS of veggies! They will be the life saver of you success. Of course, get rid of alcohol and tobacco. If you can start making these lifestyle changes NOW, you will have a much easier time after surgery. Recovery is hard enough without having to cold turkey off addictions like sugar and caffeine. Use this time to really EMBRACE the changes. Each change you make means you "WILL NEVER GO BACK!" As far as temptations go, yes they are there, but..... "IT'S JUST NOT WORTH IT!" I had to fix a full Mexican meal for a family party, make muffins for work, and cake for a birthday party. I did take a couple of tiny tastes to check for seasoning, but then I spit them out. I remind myself that my time will come to have some of these things, but not right now. Each choice you make is a choice to "go back" or "never go back." Remember that a slip up one day is a mistake. A slip up 2 days in a row is called RELAPSE. Just get back on board immediately. I found that keeping my food journal is critical. I plan all my meals (as tiny as they are) the day before, so there is no guess work the next day. We got ourselves where we are by a lot of bad choices over a long time. (Even if we thought they were good choices at the time with the dieting, starvation, and other crazy stuff we did to wreck our metabolisms and disrupt the normal hormone pathways.) It will take a lot of GOOD choices to rewire our brains and reframe our thinking about food - what is wonderful (veggies) and what is poison (sweets and simple carbs.) We can do it! Let your OCD and rules work for you!!!!!
-

Getting Banded March 4th
haroldrussi replied to tackit2's topic in PRE-Operation Weight Loss Surgery Q&A
Getting banded on 4 March as well. Stopped drinking any alcohol about 2 weeks ago (used to have a double Scotch every night) and starting the liquid diet today to try to get the liver as small and healthy as possible so I don't run into any problems during the surgery. I have read on this site where people have had to go thru the surgery twice because the liver was to big. -

ordered my first white wine
iggychic replied to Fiddleman's topic in POST-Operation Weight Loss Surgery Q&A
Fiddle, what was the restaurant. I think I know it We had a management retreat in Seattle not long after I got out of hospital and I loved the joint. I had that little chocolate ice cream with no issues For your next dining safari try RN74 downtown. It's a perfect sleeve joint as they are a tasting menu and they pace the meal well if you have more than one course. I've had no issues with anything they have served me in three trips there. Lark is also great for their small portions (tasting menu size). And I forget who asked but red wine and white wine don't differ as to how they effect your tummy. I drink both with no problem. I can drink a couple of glasses of wine without tipping over, though I'm much slower than I used to be! I've become the queen of the half glass request LOL I drink mostly white since my sleeve because the TPN really threw my palate off wack and good reds are still kind of wasted on me. I used to be able to pick out the most subtle flavors and now I just don't get them But...it's great to keep practicing LOL Some people have issues with the tannins in wines, which you'll find more of in red than white. I do find that they bother me more now than they ever did. Three glasses of red wine during a day will ensure a pounding headache the next day, but with whites I'm fine. (people say thats sulfates which is a myth...it's the tannins that are an issue). I don't know why tannins effect me now more. I should ask a wine chemist....I wonder if the high Protein diet makes a difference? We collect pinot noir so it kind of sucks! White and red wines have very low carb counts and the calories aren't bad either as long as you aren't drinking fortified wines or cheaper sparkling (where they add actual sugar to the wine). It's like 120 to 150 cals and 2 to 5 carbs per glass. I make sure to log it into my daily food intake and still don't ever go over my 800 limit. I never have gotten the instant drunk thing though. I wonder if it's because you went so long without alcohol and if that will go away? -
Hey! Hope all is well with everyone. I was just wondering, after having Gastric Bypass are you allowed to drink any types of alcoholic beverages?
-
I, too, am a wine drinker. I know it has slowed down my weight loss, but I'm still losing. I do count my wine on MyFitnessPal. I make sure I get all my protein in. I didn't have any wine for almost two months post surgery, but since then it has crept its way back into my diet. I have noticed that with greater restriction in my band, I do drink less than I did pre-surgery because there's just not enough food in my system to absorb the alcohol and I can't stand to feel "fuzzy headed". And lately there are some days I just don't have a taste for it at all.
-
My doc said alcohol is basically just empty calories, try the skinny girl line, it's good and reasonable priced, I am currently enjoying their cucumber vodka, with just water it's delicious!!! And still gives the same "relaxation" that you are looking for, the vodkas are new but they have margaritas, wines, piña colodas as well as other drinks, I swear I don't sell this stuff haha! Maybe I should though!!!!
-

Laura's RNY Journey; Age 31 Starting Weight 365
Danny Paul replied to Laura7's topic in Tell Your Weight Loss Surgery Story
My cousin is in the process of getting WLS a sleeve. He was supposed to stop all alcohol but he keeps on drinking 2 glasses a night. I told him that he wouldn't succeed if he continued to drink and if he did he would be drinking his calories. I commend you for realizing that the wine was holding you back from greater success and putting in a plan to stop it. My question, how much were you drinking on a daily basis and how much do you think it affected you getting to your weight loss goal? Thanks again for your journal and I wish you continued success. -
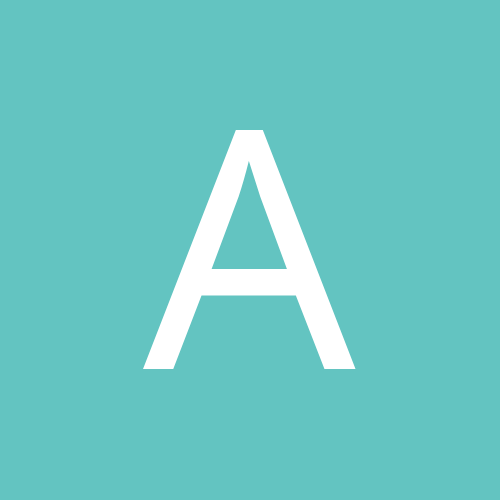
Scar healing/fading will vary from person to person. You could probably predict where you will fall on the scale by how YOU healed historically. I am on the far end of the scale of slow/bad healing/fading. I am 2+ years out from surgery and my scars are still pretty dark. They have faded somewhat from the early months (and at least now they are flat!) but they are still very noticeable (see pic below...the scars pointed at by red arrows are my WLS incision scars which are 2 years, 2 months old. My belly button is also healing from scarring from plastics 1 year ago.) Generally though, for ALL scar care, it is often recommended to keep them clean and dry while healing, and then moisturize often when they close. Also, it's recommended to reduce alcohol during healing (as it may act as a blood thinner and prevent clots), and refrain from smoking (as it may affect healing as well: stress on heart, de-oxygenates blood, etc, etc...). Further, there has been some evidence of Retinol and Vitamin E topical applications to help by stimulating collagen growth which reduces the appearance of skin imperfections.... Edited to add: Just remembered! For really bad scars, I can vouch for steroid shots. I had some applied to the arm lift scars on my arm a few weeks ago and they have visibly improved. Still not to the level of near-invisibility like i've seen on others (i'm looking at you @sillykitty), but def much better than before.
-

Band isn't working for me
cheryl2586 replied to NatalieB's topic in POST-Operation Weight Loss Surgery Q&A
The band stopping the amount of food you intake is a misconception and people need to realize it. Just because you can eat everything and as much as you want does not mean you are supposed too. Its not going to stop you from making bad food choices. You have to want this and do it. I have lost 70lbs and gving up all the things I love was worth it. Do I love to drink yes but I dont, do I love sweets more than anything but I love living even more. I could with the band sit down and eat a half gallon of ice cream and it wont stop me. I can sit and eat 10 hershey bars and it wont stop me, I can sit and eat as much food as I want and it wont stop me I have to stop myself. No one said it will be easy if they did who was it because it hasnt been easy and everyday is a daily struggle. For those who magically lost weight with no issues well yay for them because I think most people with the band struggle to maintain what they have lost and still reach for that goal. You have to want it you have to stop sabotaging yourself. Isnt the scale moving enough motivation for you. If you dont lose the weight it will eventually lose you. Your choice but make the right choice and healthy eating is not that bad it actually taste pretty darn good. As for the alcohol it wont kill you if you dont stop drinking it but it might if you dont. -

Pcp Says No Alcohol With Lap Band?
Dulci replied to horsegirl315's topic in PRE-Operation Weight Loss Surgery Q&A
My doc said that an occasional drink is ok, after the first three months. In my nutrition seminar, the dietician cautioned that a significant number of bariatric patients experience a "transfer addiction" and replace a food addiction with alcohol. -

Pcp Says No Alcohol With Lap Band?
Cocoabean replied to horsegirl315's topic in PRE-Operation Weight Loss Surgery Q&A
I have beer from time to time. I find it easier to drink than soda. It will sometimes give me the hiccups. Which is terribly embarrassing. Sipping one beer and HICCUP! Oh well. I just recently went to one of my surgeon's support groups (surgeon was not there). A patient going through screening says his nutritionist is now saying alcohol is ok 1 year post-op. I cannot remember what he told me this late in the game. -

im 9 days out and I ate 5 hot cheetos
Heyher replied to dee2rod's topic in POST-Operation Weight Loss Surgery Q&A
I agree chicken broth or tea. If you are looking for something more sweet diluted G2. But I have to ask why flaming hot Cheetos? The thought of anything remotely spicy that early out... Reflux, excess stomach acid, fresh wound in the tummy... I would think it would feel like swallowing rubbing alcohol. -
Oh, wow was this a good read folks!!! Hope all works out BG. I love tomatoes, have about 24 ounces of coffee a day (it is a lot huh) I know and not much citrus or alcohol. I have started slowing down even more my 1/2 a cup of food (4 ounces) takes me over a half an hour to eat. It is crazy? I just have to go really slow or I get stuck. I chew like a COW, I sometimes swallow only half of what is in my mouth and then wait and swallow the rest in a few seconds. I have been drinking the water trying to get it all in, but it is hard. I have been having the other kind of gas. The other end. LOL. You just can't take me anywhere I blame the dog!! Maybe it is what I am eating that gives me the gas? I do not burp at all and I never have. If I try to burp more than air comes up usually. I may be saying just a little too much here. Sorry..... I just love your blog BG you are the best Made any soup lately? Have a nice night. imaluckydog
-

No alcohol ever?!
Angie74 replied to nervousnelly719's topic in PRE-Operation Weight Loss Surgery Q&A
Same but I have friends who have had it done and occasionally they enjoy a nice beverage. However they get tipsy much faster and it goes away faster. Once u get healthy I'm sure u won't want to drink much, plus alcohol puts weight on Sent from my SAMSUNG-SM-N900A using Tapatalk -
I enjoy alcohol when I go out on weekends. I'm 4 months and my surgeon is okay with it. I used to be a big beer lover. More accurately....i was just BIG....and loved beer. lol. Now, I drink high grade liqueurs with low calorie mixers. I try to avoid anything carbonated. If I'm mixing something at the house, then I"ll use a really good vodka or tequila mixed with Ocean Spray Diet Cranberry (5 calories per serving) over ice. Smooth and tasty. Prior to surgery when I'd go out....I didn't do well with nursing a beer....it was normally 6-8 beers with some tequila shooters over the course of an evening. Watching a football game at a sports bar.....more than that. Now....a couple of those "skinny" liquor drinks and I'm good to go. I had this surgery to improve my health....and quickly. I'd have agreed to anything.....any terms or conditions in order to do that. What happened over the course of these 4 months post-op, though, has been much more than simply my health being improved.....but my state of mind as well. I truly enjoy every aspect of life in ways that I'd just forgotten about. Going out and having fun with others.......or just lone-wolfing it and flirting with a hot bartender or two.....fun stuff that helps in many ways. It's almost therapeutic. If having a few occasional drinks is fun......then so be it. I didn't have this surgery to live like a monk. I did it to feel better......and feel better, I shall. Hell.....two weeks ago....one of the gals on the surgeon's staff...who was a tremendous help with me getting throughout my pre & post op.....met me for a couple pitchers of skinny margaritas. We had a blast and were able to laugh about all the crazy stuff related to my case and then with her job. Fun stuff. I seriously doubt she would've bought the second pitcher had she been worried about it hurting me.......thusly, I consider it part of my ongoing care when we do it again. All things in moderation...........